


The possibility of autonomous Buurtzorg care teams across the UK: tantalising hope vs organisational rigidity (Part 1)
A senior NHS leader asked me whether Buurtzorg's self-managed/Teal community care approach - such an inspiring success in the Netherlands - exists in UK healthcare. Here's what I uncovered...

1. The spread of Buurtzorg-inspired organisations across the UK
2. What stands in the way? Hard lessons from Britain’s Buurtzorg pioneers
3. Other self-managed organisations
4. Are NHS Integrated Care Systems (ICSs) an opening for self-management?
Setting the scene…
Back in 2014 Frederic Laloux self-published Reinventing Organizations. Its appealing descriptions of a range of productive and purposeful organisations that have been built on self-management, rather than hierarchy, turned it into a surprise hit. It has since sold approaching a million copies, with translated editions around the globe. One particularly memorable organisation included was a Dutch community nursing organisation, Buurtzorg, founded in 2006 as a team of four nurses who were disgruntled at what the home-care sector had morphed into – too much bureaucracy with too little autonomy.
Some months back a senior NHS leader who – like me – felt inspired by Laloux’s book asked me whether, or even if, these approaches – such as Buurtzorg’s – are being taken up within UK health and care.
Rather than replying with a few quick sentences based on what I already knew, it quickly dawned on me that I really wanted to get to the bottom of where the UK is now with such person-centred autonomous team approaches – given what a positive change they could make to today’s often impersonal, transactional services. Is a radical shift to less hierarchical, more human, organisations possible in the NHS and beyond? And – more importantly – is this transformation already happening out there?
Although I have myself in the past worked in a couple of small self-managed organisations (relatively briefly), and once even co-founded a website, Enlivening Edge - News from Next Stage Organisations, all about these organisations, by now I was back working within a conventional hierarchy and, basically, rather out of that loop.
So I launched myself into trying to uncover – as quickly as I could – a picture of self-managed organisations in health and care round the UK. I can’t guarantee that my quick picture is truly comprehensive (nb I’m happy to retrospectively add in any other organisations etc that I may have overlooked – please let me know!).
Nevertheless here’s a first stab at seeing what’s been going on out there: the good, the bad and the ugly. The many trials and tribulations of being on the leading edge of a shift to more human – less machine-like – health and care. And – perhaps inevitably – at least some grappling with the million-dollar question: do these new organisations – when they do spring up – really hold out the potential to transform significant parts of the UK health and care system for the better?
Yet as the possibilities of a more community-based, relationship-building, strengths-based and less bureaucratic health and care future gradually became more visible, the lack of receptiveness of today’s NHS and related care structures to such changes soon forced its way onto the agenda as a central issue. (In part 2 – coming soon – I also ask whether there exist out there worthwhile stepping stones in the direction of autonomy and shared power in health and care, when full self-management is just not currently a realistic proposition. In other words, is there anything we can do in the organisations most of us are at work in today that might bring us closer to these autonomous and self-managed teams?)
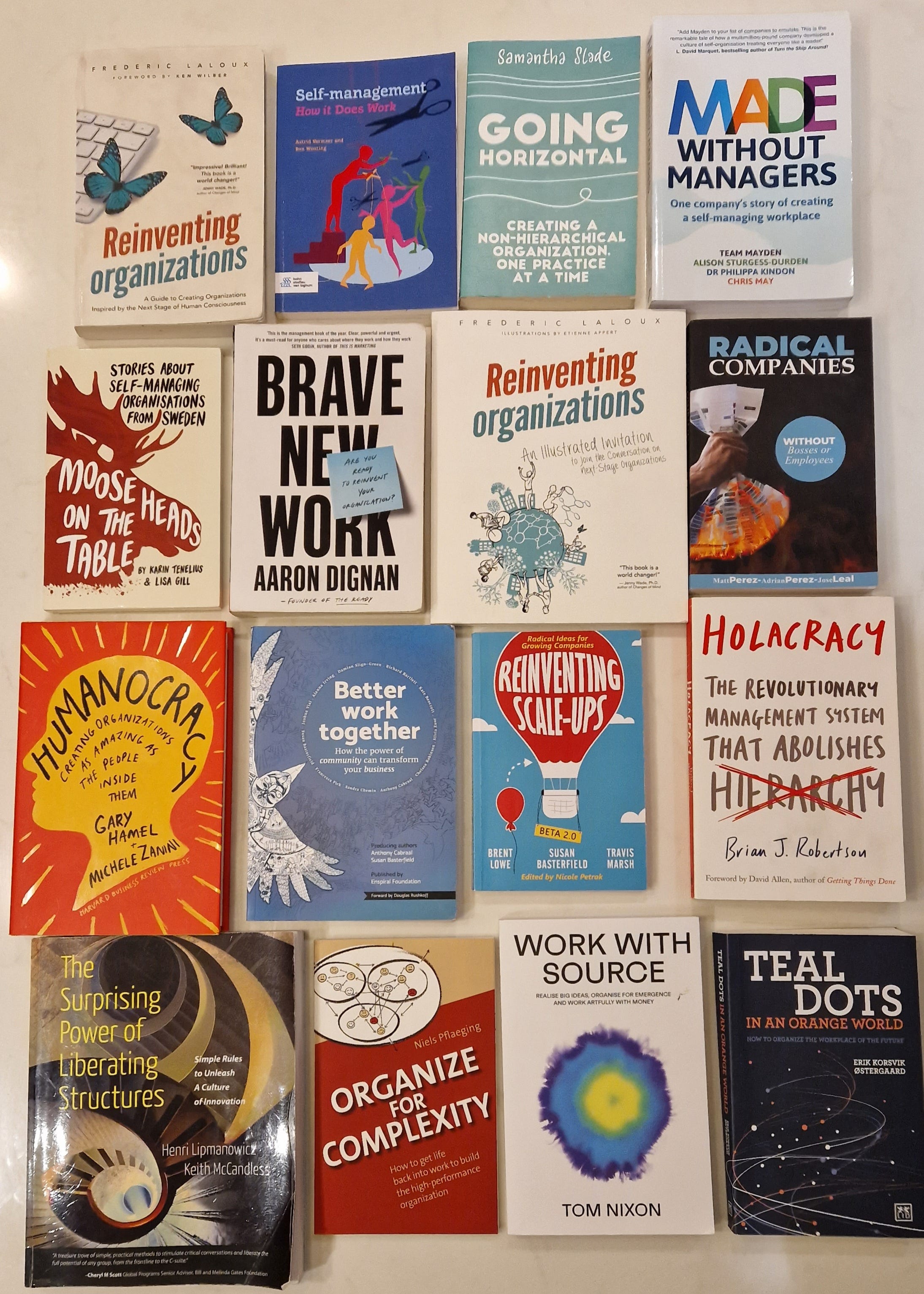
The NHS and related developments I’ll be discussing below are just one part of a much larger movement: here’s a selection of recent books about self-managed organisations. Reinventing Organisations was the surprise bestseller that helped popularise the stories of Buurtzorg, Morning Star and others (there’s a shorter illustrated version too). Self-Management - How it Does Work is a short practical guide to running Buurtzorg teams. Made Without Managers - one company’s story of creating a self-managing workplace shares the story of a UK software company working with the NHS.
Radical Companies - without Bosses or Employees brings attention to the related issue of co-ownership too (just to complicate things, the historic standard-bearer of co-ownership, Spain’s Mondragon, doesn’t itself really use self-managed/non-hierarchical structures!). Going Horizontal - Creating a non-hierarchical organisation, one practice at a time is a practical guide to tools and methods for self-managed orgs (such as Generative Decision Making). Liberating Structures - Simple Rules to Unleash a Culture of Innovation isn’t a self-management book per se, but shares 33 fabulous and fun creative group tools that any team or organisation can use to give everyone a voice in sharing learning, unleashing local action, spreading innovations etc. I include it as many self-managed orgs have found them invaluable (and their use is spreading impressively in the NHS, as discussed in part 2.)
1. The spread of Buurtzorg-inspired organisations across the UK
Thanks in part to Frederic Laloux’s book Reinventing Organisations – A guide to creating organisations inspired by the next stage of human consciousness, Buurtzorg neigbourhood care’s success in the Netherlands is increasingly well-known over here – and it’s surely the prime example of a ‘Teal’ self-managed approach in UK health and care too. (The somewhat contentious use of the colour label ‘Teal’ to describe these novel organisations is discussed in part 2).
The short version of what this means in reality is that Buurtzorg has 16,000+ community nurses and care-givers in the Netherlands, supported by a tiny national head office staff of under 100 people. There are just two managers, for the 900+ teams (of up to 12 nurses each), meaning they all have a high level of autonomy to control their day-to-day work. In lieu of managers, the team can draw on support from 22 regional coaches, if needed – who have an enabling role, not a management role.
Cambridge University business academic Mark Thompson, writing in the Guardian in 2015, commented when he first heard about Buurtzorg that it “made me fall off my seat”. He made a back-of-the-envelope calculation that this self-managed approach could save £35.5bn across Britain’s public sector, freeing up thousands of staff to return to valuable frontline work.
Buurtzorg co-founder Jos de Blok told me the Dutch Health Ministry had found that the Buurzorg self-management model could potentially spread to up to 30% of health and care services.
Here’s how Buurtzorg describes itself:
“Buurtzorg is a pioneering healthcare organisation established in 2006 with a nurse-led model of holistic care that has revolutionised community care in the Netherlands.
“Client satisfaction rates are the highest of any healthcare organisation. Staff commitment and contentedness is reflected in Buurtzorg’s title of Best Employer (4 out of the last 5 years). And impressive financial savings have been made. Ernst & Young documented savings of around 40 percent to the Dutch health care system, and a KPMG Case Study in 2012 found:
“Essentially, the program empowers nurses (rather than nursing assistants or cleaners) to deliver all the care that patients need. And while this has meant higher costs per hour, the results have been fewer hours in total. Indeed, by changing the model of care, Buurtzorg has accomplished a 50 percent reduction in hours of care, improved quality of care and raised work satisfaction for employees.” (Patients are also reportedly less likely to be admitted to emergency departments and when they are admitted, they are more likely to have a shorter hospital stay – reducing pressure on the health system).
“Buurtzorg scaled very quickly across the Netherlands from 1 to 850 teams. During this time Buurtzorg grew in other areas of care such as mental health, children and families and also supported other Dutch international care organisations to take on the Buurtzorg model of care.”
Transforming an NHS, or community care, team into an autonomous, self-managing team – like Buurtzorg’s teams – will typically need basic work done on team dynamics, moving away from the unhealthy Parent-Child type of dynamics which are so prevalent as to be almost accepted as normal in conventional organisations.
Sometimes key foundations of Buurtzorg’s approach in the Netherlands can be so deeply integrated into its work that they can end up almost invisible to outsiders like us in the UK (and the 23 other countries that have already partnered with Buurtzorg). For example, Buurtzorg encourages an ‘Intervision’ – rather than supervision – process with staff, which encourages ongoing reflective practice and a solution-focused approach.
‘That in some ways’, explains Buurtzorg Britain & Ireland Managing Director Brendan Martin, “is the core of the whole thing”.
“But it was so embedded in Buurtzorg norms that we almost didn’t see it. In the NHS you really have to be explicit about it”.
The work of Buurtzorg Britain & Ireland – across 40 different settings

Buurtzorg Britain & Ireland is Buurtzorg’s approved partner for the UK. Managing Director Brendan Martin shares their story: “When we began our partnership, Buurtzorg founder Jos de Blok and I agreed that our aim was (and remains) to support system change, and we both had a lot to learn about the British system. For the time being, therefore, we then decided not to found a British equivalent of Buurtzorg as a service provider. Rather, we would work to support existing NHS, social care and other organisations in Britain and Ireland to change the way they provide services, organise work and support their workforces, drawing on Buurtzorg’s experience and applying the principles behind its success.”
There has been significant take-up since that start: “We have now done that, in small and larger ways, in around 40 settings across Britain and Ireland. These projects have included ‘test and learn’ experiments in setting up and supporting self-managed teams, such as at Guy’s & St Thomas’s NHS Foundation Trust and with Healthcare Improvement Scotland”.
Buurtzorg at Guy’s & St Thomas’s NHS Foundation Trust – the nurses’ experience
An adapted version of Buurtzorg – known as Neighbourhood Nursing - was run as a pilot from Nov 2016 to – June 2017. The pilot was then extended until June 2019.
We found great satisfaction in the type of patient care we could offer and in being a team with members of equal status
- Guy’s and St.Thomas’s neighbourhood nurses
A November 2022 article in the Journal of Community Nursing, by three members of the Guy’s & St Thomas’s teams reports: “We found great satisfaction in the type of patient care we could offer and in being a team with members of equal status”.
They “received so much positive feedback from patients, their family members, GPs, allied health professionals and specialist teams”.
“They… were often able to tell us that while a previous experience of the district nursing service was good or OK, this was better.”
“We knew what we were doing was different,”’ the three authors explain, “as we had previously worked in district nursing services where the focus was so often on a single clinical task to the detriment of seeing the bigger picture for that person.”
“The named nurse concept made it so that you could follow your patient’s journey, and ensure that they were signposted to the right teams at the right time.”
Working in this self-managed Neighbourhood Care team “contrasted with our experience in traditionally organised district nursing teams where each staff member had their list of patients for the shift and the responsibility was theirs alone.”
“In those teams there was no sense of collective problem solving or helping each other to complete the necessary work in that shift”.
There were plenty of challenges to working as a self-managed team, linked to being part of a large trust. For example everything needed a manager’s sign-off – which meant they could not respond in timely ways to patients’ needs. NHS’s IT was ‘cumbersome’ compared to what Buurtzorg had developed, seeming to be “time-consuming with little use to our nursing care”.
‘The time and task model prioritises procedures (tasks) and the amount of time spent on care over meeting the needs of individual people’
- Karla Zimpel-Leal
They concluded from their experience that this Buurtzorg-inspired approach “has much to offer with its attention to the patient at the centre and concern for giving control to the nursing staff in finding the best ways of working for them and their patients.”
(It’s worth highlighting the mention above of how conventional services will often focus on a single clinical task, the so-called ‘time and task’ model. It will come up repeatedly. Karla Zimpel-Leal describes it well: “The time and task model prioritises procedures (tasks) and the amount of time spent on care over meeting the needs of individual people”).
The Buurtzorg work has continued at Guy’s and St.Thomas’s – though not spread further in that Trust, in the way one might have hoped it would.
Healthcare Improvement Scotland (HIS)
Healthcare Improvement Scotland supported a range of partnerships – inspired by Buurtzorg – to test models of neighbourhood care.

They explain the Buurtzorg model like this: “The model was developed in response to a fragmented landscape of home care provision in the Netherlands, in which people were receiving care from multiple practitioners and providers.”
“Rather than carrying out fixed tasks for people in isolation, the Buurtzorg model takes a holistic approach and looks at what patients and service users can learn to do for themselves again, reducing the need for care in the future.”
“Its focus on neighbourhoods allows teams to use informal networks and work together with a range of professionals, such as GPs and pharmacists, and to engage in preventative activities.”
(NB Beveridge’s prediction, at the founding of the NHS, that the need for care, and thus costs, would reduce quickly proved very wrong. Using the Buurtzorg approach, this reduction in need for care actually does happen over time).
The partnerships were:
NHS Highland
Aberdeen City HSCP
Scottish Borders HSCP
Clackmannanshire & Stirling HSCP
Western Isles HSCP
Argyll & Bute HSCP
Cornerstone
One of the projects, Cornerstone, has been one of the largest organisations supporting self-managed teams – managing to retain all their previous contracts during their transition to self-management, as well as winning new ones.

Their then CEO Edel Harris explained – in the 2018 publication Insights for a Better Way – Improving services and building strong communities – the current state of social care which they seek to transform: “Over recent years, with the emphasis on austerity and the resulting public service funding crisis, the social care sector in the UK has become an industry that in many cases has lost the focus on the person requiring care and support. Time and tasks have become the order of the day with often stressed, low paid workers following a schedule and a set of rules that have more in common with a manufacturing production line.”
And the new Buurtzorg-inspired ‘Local Cornerstone’ approach they aim to replace it with?: “Can you imagine a workplace with no managers, no supervising and checking, no burdensome policies and procedures, three simple measurements and a network of up-skilled, local, self-managed teams all focused on achieving a charitable purpose?”
“Cornerstone is changing its culture to remove hierarchy, replace traditional management with a coaching approach and by stripping out unnecessary policies and procedures we are trusting people to do the right thing.”
“We only recruit and retain the very best people by hiring for values. We are improving staff retention and happiness by demonstrating our appreciation of the wonderful work our colleagues do and by allowing team members to manage their own workload. By reducing our central overheads and as a result of a significant investment in technology we have managed to do all of this in a financially sustainable way.”
“Throw away the rule book,” she exhorts.
‘No one wants their legacy to be that they met their KPIs’
– Edel Harris
“Recruit and retain the best people with the best attitude. Value them and trust them to do a good job. Remove the obstacles that are in their way and challenge regulation and contract compliance when you believe it is contrary to the outcome you are trying to achieve.”
“No one wants their legacy to be that they met their KPIs – we are driven by a sense of purpose and a desire to make a difference”.
Though the latest information will be different, at one point they had 31 self-managed Local Care and Support teams, supporting 2,700 patients annually. Autonomy and accountability was devolved to the frontline – resulting in a 40% reduction in overheads.
Their plan was to move the whole organisation across to 110 self-managing teams. There would then be an evaluation (funded by Big Lottery Scottish Government and the Carnegie Trust). They have found that NHS commissioning restricted their model.
Cornerstone’s CEO Edel Harris later left to become CEO of Mencap, the UK’s largest charity working with/for people with a learning disability. There she hoped to get Mencap to adopt similar approaches, though slightly different from the Buurtzorg model she developed in Cornerstone. Work begun there slowed, however, as the Covid era was not an optimal time for attempting such a radical shift.
(Unconfirmed rumour has it that Cornerstone has begun to edge back towards a more conventional structure since Edel departed).
Interestingly, running into Edel at the June 2023 NHS Confederation conference, she told me she personally avoids ‘self-managing’ as a label, preferring the term – ‘place-based autonomous teams’. The reason being that the former can wrongly leave many managers with the feeling there won’t be opportunities for them when an organisation transforms towards a more autonomous structure: a scary prospect. She was still viewing place-based autonomous teams as her ultimate aim at Mencap, which she recently left, though felt the time wasn’t right to try it, in the way it had been for Cornerstone.
As with Guy’s, significant challenges were encountered to this new way of working.
The ‘Learning from neighbourhood care test sites in Scotland December 2019’ evaluation shared that: “Staff reported a number of challenges relating to the implementation of neighbourhood care principles and the development of new models within complex health and social care settings. These included difficulties for teams becoming self-organising and difficulties for professionals to work outwith traditional boundaries.”
“Additional reported challenges were lack of supporting systems, infrastructures and resources, bureaucracy, workforce sustainability issues, complexity of caseload and expectations.”
Plenty of positives – of potential – was seen too. A Neighbourhood care team staff member, in Kintyre in Argyll and Bute, said “We’re already seeing a reduction in delayed discharge – and having these results has really helped to maintain the momentum”.
Other evaluation work by the ihub of the Forres neighbourhood care team in Moray also illustrated that the model may reduce hospital admissions with associated efficiency savings.
In Forres, evaluation findings “suggest that there are signs that the FNCT [Forres Neighbourhood Care Team] may begin to impact on hospital emergency admissions in the Forres area. For those people cared for by the FNCT there is some evidence of reduced costs associated with hospital admissions (reduction in number of admission and length of stay).”
The cultural challenge to conventional hierarchical management structures shouldn’t be downplayed. One anonymous Neighbourhood Care team staff member commented: “Staff were informed that they could design a model that fits the area, unfortunately senior management would not accept this model and introduced an alternative.”
‘Staff were informed that they could design a model that fits the area, unfortunately senior management would not accept this model and introduced an alternative’
- Anonymous Neighbourhood Care team staff member
Looking across all the seven partnerships in Scotland, an HIS team member commented that it felt like “Lots of things that started but they hit the system and the feeling being very much like the proverbial ‘brick wall’. Certainly within the public sector structures not enough was done to create the wider system changes (job titles and roles, flexibility to work across organisations in a meaningful way etc).”
Commissioning in particular causing a problem as it (in its current form) is not effective at realising the benefits of a Buurtzorg type model
“Commissioning in particular causing a problem as it (in its current form) is not effective at realising the benefits of a Buurtzorg type model.”
The partnerships ran from March 2016 to March 2019 – but have not continued in that form since. That’s not to say that HIS isn’t trying to take forward their learning from Buurtzorg-inspired neighbourhood care and other community-led models. They’ve been working alongside the Community-led Support model over the past five years, and more recently developing Prof Toby Lowe’s ‘Human Learning Systems’ approach in Scotland.
They are also addressing the commissioning barriers to collaborative practice (one of the things that restricted the Cornerstone model).
This ‘Commissioning Differently’ work aims to change current commissioning practice that is “focused on purchasing services which are utilised to look after people who are deemed vulnerable and ‘qualify’ for support under strict eligibility criteria. This is a deficit model and people are allocated their portion of a limited resource. This model also encourages a dependency culture.”
“The Adult Review of Social Care clearly sets out the vision of moving to a more person-centred, collaborative, trust-based and ethical way of commissioning within health and social care.”
Significant change is demanded: “All public sector organisations will need to develop new models of commissioning and procurement that are fit for purpose within their local context in preparation for what’s ahead including the National Care Service.”
Des McCart (Senior Programme Manager, Healthcare Improvement Scotland) concludes that in Scotland “We are very much still on the journey towards more sustainable models of health and social care based on similar elements as were seen in Buurtzorg”.
“We are looking at the wider structural changes required to do this – and indeed, more importantly, the relational changes that are required also.”
Though the pilots may not themselves have thrived and spread widely, as can often happen experience using the Buurtzorg approach may reappear later, or in related places. For example Aberdeen City Health & Social Care Partnership’s leadership team – inspired by its local Buurtzorg pilot – has chosen to operate in a flat, distributed structure since 2019. The impacts on staff satisfaction, autonomy, collaboration and creativity have been very positive (see Leask and Macleod, 2023).

Longer-term radical organisational change
“In a few places we have gone on to support long-term radical organisational change”, explains Brendan, from Buurtzorg Britain & Ireland, “such as with the Thistle Foundation in Scotland, and Medway Community Health in Kent as part of an EU-supported Transforming Integrated Community Care (TICC) project.” (See video of the final conference of this 4-year pan-European project, in November 2022).”

The Thistle Foundation is the largest Buurtzorg-inspired development in the UK, with 20 teams currently (and now working to change its back-office too). Medway has reached a significant size too, with a total of 12 self-managing teams.
“Examples of such long-term radical organisational changes are few but significant because they depend on robust long-term leadership commitment to making the organisational changes required to grow and sustain a new approach.”

Even when a Buurtzorg-inspired experiment in self-management doesn’t continue – as in places like Cambridgeshire, West Suffolk (see evaluation) and Tower Hamlets – it doesn’t necessarily follow that there has been no impact, that the inspiration to try a new and better approach has been permanently lost. Members of self-managing teams that have stopped and find themselves redeployed may end up spreading their learning into the mainstream of an organisation (this seemingly has parallels with the phenomenon Michael Arena noticed of centralised innovation teams that have zero effect, up until they are redeployed back across their organisation; see Adaptive Space – how GM and other companies are positively disrupting themselves and transforming into agile organisations, 2018, page 22).
It can be a long game: “We plant a seed, forget about it, and three years later they come back”, explains Brendan.
Other places that Buurtzorg-inspired work is taking place in include Dorset and Cheshire (“Our teams have adopted "Buurtzorg" principles”).

2. What stands in the way? Hard lessons from Britain’s Buurtzorg pioneers

Brendan draws on Buurtzorg’s UK experience along with the evidence of independent evaluations of several of their projects to gauge the current situation: “Health and care professionals in Britain have shown themselves just as capable as their Dutch counterparts of working in the Buurtzorg way, and having done so seldom wish to revert. The people they serve have also seen the benefits in more timely, co-ordinated holistic care.”
‘Health and care professionals in Britain have shown themselves just as capable as their Dutch counterparts of working in the Buurtzorg way, and having done so seldom wish to revert’
– Brendan Martin
“But their organisations, with few exceptions, have not been able to make the practical, cultural and structural changes needed to support them well at scale. Without doing that they are unable to grow and sustain the early benefits and secure the financial savings the model has demonstrated in the Netherlands.”
“We are currently analysing more than 250 particular ‘barriers and challenges’ identified by our partners in the Transforming Integrated Care in the Community (TICC) project in Kent and France, and these align well with our broader experience in Britain and Ireland.” (See section below for more on this EU Buurtzorg report).
‘But their organisations, with few exceptions, have not been able to make the practical, cultural and structural changes needed to support them well at scale’
– Brendan Martin
A key goal of TICC is to understand and “overcome blocking points in transferring socially innovative service models from one area to another” – highly relevant for understanding Buurtzorg’s challenges in the NHS.
The obstacles in the NHS and care system
Buurtzorg Britain & Ireland’s analysis sees the obstacles in four categories:
Barriers and challenges related to applying the Buurtzorg model in institutional contexts in which Buurtzorg values, culture and goals are not widely shared or promoted.
Barriers and challenges facing community nursing generally within the national context.
Barriers and challenges relating to innovation generally.
Barriers and challenges relating to the model itself.
Teams were trying to work in a holistic, patient-centred way but dealing with regulatory and monitoring systems that did not support this
The first category was by far the most prevalent and manifested in four related ways:
a) Inconsistent organisational goals meant that teams were being funded and monitored according to indicators that did not reflect the outcomes they were trying to work towards within the Buurtzorg model.
b) Lack of integration of services at all levels meant that teams were trying to work in a holistic, patient-centred way but dealing with regulatory and monitoring systems that did not support this. Funders and regulators divided work up according to type of care (health or social) and geographical boundaries that did not match the neighbourhoods served.
c) Hierarchy and competition within institutions had the effect of undermining the professional autonomy of the teams, obstructing their work and making it harder for them to operate in a non-hierarchical and collaborative way.
d) Systems-led working meant that teams were often required to adapt their work to fit inflexible institutional systems, rather than systems being designed to support the purposes of their work.
Hierarchy and competition within institutions had the effect of undermining the professional autonomy of the teams, obstructing their work and making it harder for them to operate in a non-hierarchical and collaborative way
Next steps for Buurtzorg Britain & Ireland
Drawing on their experience so far, their planned next steps to overcome these challenges have three elements:
1. Continuation of our current work of providing learning and development support to NHS, social care and other organisations wishing to make changes inspired and informed by the Buurtzorg model.
2. Creation of a joint venture with suitable partners to build a Buurtzorg UK social enterprise to provide holistic health and social care in community settings within one or more Integrated Care Systems.
3. Development, in partnership with an IT partner, of a digital platform that will match people wishing to access care and support with providers willing to adopt the Buurtzorg approach and accept our quality assurance processes as a condition of joining the platform.
Paul Jansen, who previously worked for Buurtzorg Britain & Ireland and now runs his own self-management training organisation, Trust Works, has blogged about the barriers he sees to implementing self-management in the NHS here: Lessons from going Dutch in the UK’,
He offers some further suggestions on why the hoped-for scaling up doesn’t happen, and why promising Buurtzorg teams often get absorbed back into their traditional host organisations.
“We have seen teams of nurses and homecare workers thrive as self-managed teams. And we have seen patients flourish under their care and make remarkable progress”, says Paul.
“Nevertheless, full take-up of the model has not quite happened (yet), and many promising teams have been absorbed back into their wider organisations. More successful pilots have at best continued, but without fully scaling up throughout the wider organisation.”
Paul suggests there are 4 challenges:
Challenge 1: Is there a paradox in following a good example?
Organisations like Semco, Patagonia and Buurtzorg had a clarity of purpose when they started out, but their transformation was more in the journey than the destination, as there was no clear end-point.
‘There is a risk that being inspired by one such example and wanting to replicate its model because of its great outcomes, will divert your transformation process away from your own journey and into the path of ‘implementing’ your source of inspiration into an environment which isn’t quite suited or quite ready for it'
- Paul Jansen
Will models like Buurtzorg ‘stick’ if organisations don’t go through a similar process?
Paul warns: “there is a risk that being inspired by one such example and wanting to replicate its model because of its great outcomes, will divert your transformation process away from your own journey and into the path of ‘implementing’ your source of inspiration into an environment which isn’t quite suited or quite ready for it.”
’Often people want a silver bullet – to be able to take a successful initiative from one place and replicate it in their own. In reality, this rarely works. It is like breaking off the tip of an iceberg and trying to get it to float somewhere else, without the structure below that underpins it. That is because the real change is not the new initiative per se, but the learning and consequent transformation of people, relationships and systems which gave rise to the particular initiative’
– Celia Carrington
“Don’t copy a model wholesale and expect it to work for you”, he adds.
I like Celia Carrington’s similar warning about this ‘silver bullet fallacy’ (from a 2015 report Reducing Dependency on Place-based Services): “Often people want a silver bullet – to be able to take a successful initiative from one place and replicate it in their own. In reality, this rarely works. It is like breaking off the tip of an iceberg and trying to get it to float somewhere else, without the structure below that underpins it. That is because the real change is not the new initiative per se, but the learning and consequent transformation of people, relationships and systems which gave rise to the particular initiative.”
Challenge 2: How to lead while not knowing where you’re heading?
People will see the shift as a minor change, or just another fad, if you as a leader “act the same, demand the same performance measures, ‘do change’ in the same way as usual,” writes Paul.
‘You have to be prepared to experiment, to let go, to trust, to support to make mistakes, to be patient’
– Paul Jansen
“Self-management is about unleashing the intrinsic motivation of people for the benefit of the organisation and its customers. That requires clarity of purpose, autonomy and a thirst for learning. If you want self-management to stand a chance of succeeding, you – the leader – will have to change your behaviours, your language and your leadership style accordingly.”
“You have to be prepared to experiment, to let go, to trust, to support to make mistakes, to be patient. In short you must create safety in the organisation to allow for the change to take shape”.
Explore successful examples like Buurtzorg, advises Paul, but with the focus on learning from their journey and leadership lessons rather than the technical specifics of their particular solution. Work with your own organisation for clarity on your primary purpose and what the design principles should be for “a more self-managed future version”.
‘[Most UK Buurtzorg teams] functioned really rather well and achieved results not dissimilar to Buurtzorg itself: very happy patients, better clinical outcomes, and higher levels of engagement and retention amongst the care professionals’
– Paul Jansen
Challenge 3: the dual paradigm issue
In the UK, efforts have been made to create a small number of self-managing teams: “we tried to create a bubble where different rules of engagement applied”. A senior figure would often act as a ‘heatshield’ person.
Most of these pioneering teams, once settled in, “functioned really rather well and achieved results not dissimilar to Buurtzorg itself: very happy patients, better clinical outcomes, and higher levels of engagement and retention amongst the care professionals,” says Paul.
But projects continued to struggle with the interaction with the wider organisation.
“Despite the heatshield, getting the organisations to support the teams in line with their needs as well as their – admittedly unusual – rules of engagement, appeared beyond their capability”.
‘I fear that organisations that work on the basis of a paradigm of control, hierarchy and administrative oversight cannot also – and at the same time – operate on a self-management paradigm based on trust, devolvement and support… I now believe a hard separation will be required in order to be successful’
– Paul Jansen
Examples included the inability of teams to order medical devices or IT equipment ‘because there is no manager sign-off’, interventions by middle manages that undermined trust in the teams and imposition of standards and processes that teams believed undermined their autonomy.
Could such challenges be overcome? Well, most organisations decided not to proceed with their Buurtzorg projects before this could happen.
Paul concludes: “I fear that organisations that work on the basis of a paradigm of control, hierarchy and administrative oversight cannot also – and at the same time – operate on a self-management paradigm based on trust, devolvement and support”.
It’s like an iPhone trying to run an Android app.
“I now believe a hard separation will be required in order to be successful’ – ie by spinning out the Buurtzorg-based service as a separate entity. (This echoes one element of Buurtzorg Britain & Ireland’s planned way forward: ‘a joint venture with suitable partners to build a Buurtzorg UK social enterprise’).
“There is no reason why this entity could not be (co-)owned by the original service.”
Challenge 4: Can self-management be done at scale
‘The jury’s still out’ on whether self-managed models can grow to scale in the UK health and care sector.
‘If you are part of a much larger organisation and are at risk of being dominated by its legacy structure, culture and processes, consider creating a separate entity for your self-managed service. Only then are you likely to be able to escape the gravity pull of the mothership’
– Paul Jansen
Though evidence shows that such self-managed organisations can be large – Buurtzorg has 16,000+ employees in the Netherlands and Chinese white-goods producer Haier has around 100,000 employees. And General McChrystal’s book Team of Teams showed how the US Army was transformed onto a network-based footing – rather than command-and-control – in the midst of the Iraq war.
Buurtzorg has also supported successful transformations of other organisations with up to 2,000 staff, in the Netherlands.
Exactly as Buurtzorg Britain & Ireland are now seeking to do, Paul suggests: “If you are part of a much larger organisation and are at risk of being dominated by its legacy structure, culture and processes, consider creating a separate entity for your self-managed service. Only then are you likely to be able to escape the gravity pull of the mothership and create the right environment where all components move in the same direction”.
Beyond Paul’s four challenges, additional more specific challenges include the savings that a Buurtzorg approach can enable not being made in the part of the system that commissioned the work but elsewhere in the system, which sadly doesn’t count when decisions on funding to continue a Buurtzorg project are made. One project even had a budget for evaluating its Buurtzorg-based work that was twice as high as the budget offered to Buurtzorg for the self-management learning and development of the teams in the first place.
New EU report about whether Buurtzorg can spread: finds 250 barriers – but solutions too

The 2023 Transforming Integrated Care in the Community (TICC) report – across 4 European countries – highlights almost 250 different barriers to the successful spread of a Buurtzorg approach.
It also made clear its appeal: “[Buurtzorg] became an international exemplar of a form of work organisation based on valuing and mobilising the intrinsic motivation, knowledge and experience of professionals by enabling and supporting them to work in self-managed teams with high levels of freedom and responsibility”.
‘[The 1990s ‘New Public Management’ reforms sought] to define and standardise specific service tasks required to achieve a policy-driven result, to cut costs by assigning them to the lowest price provider and to hold public service workers accountable in a strict performance management regime… In the Netherlands the result was that costs doubled in ten years while service quality fell’
“Its success has found expression in well-evidenced and sustained improvements in the quality of care it provides, the job satisfaction experienced by its staff (and their retention) and cost reduction”.
The last 20 years, the report explained, have seen changes that were intended to improve care but actually “led to the fragmentation of care, a task-driven, activity-based approach, and less efficient resource use.”
More specifically, the 1990s, in many countries, saw a series of public service reforms often referred to as ‘New Public Management’: “the drive was to define and standardise specific service tasks required to achieve a policy-driven result, to cut costs by assigning them to the lowest price provider and to hold public service workers accountable in a strict performance management regime”.
‘Patients would be seen by a procession of different professionals and providers, each of whom was responsible for a different aspect of their care, none of them spending more than a few minutes in their home. Patient satisfaction declined , and the nurses themselves became increasingly demotivated to the extent that many left the profession’
“In the Netherlands the result was that costs doubled in ten years while service quality fell.”
“Patients would be seen by a procession of different professionals and providers, each of whom was responsible for a different aspect of their care, none of them spending more than a few minutes in their home. Patient satisfaction declined, and the nurses themselves became increasingly demotivated to the extent that many left the profession”.
The report concluded: “[T]he experience of the project suggests that the main obstacles to the application of the Buurtzorg model outside its country of origin arise not from any inability of nurses outside the Netherlands to operate with high levels of autonomy, but from organisational and systemic failures to support them in doing so.”
Here are a few snippets from amongst the litany of challenges:
Teams are focused on outcomes whilst being funded for tasks completed
Senior managers struggled to allow teams to have autonomy
A pervasive competitive system or culture undermined teams’ ability to work collaboratively toward the purpose of the Buurtzorg goals.
“A plethora of reports and KPIs we are obliged to collate and submit to our NHS commissioners”
“The model requires teams to be located in neighbourhoods – commissioning currently aiming to centralise all teams in Healthy Living Centres”
One partner continued to refer to staff by their NHS band number.
But, fortunately, the report’s 239 pages of challenges comes with solutions and outcomes for almost every single one identified.
These barriers and reversals faced by Buurtzorg-style teams are – sadly – far from unexpected. There have been many experiments, even movements, towards more participative management over the years. For example, Eric Trist’s Sociotechnical Systems (STS) in the 60s and 70s encouraged small, self-managing teams. It would see General Foods set up a plant in Topeka, Kansas, that proved influential, setting new benchmarks in every area of performance, Gary Hamel and Michele Zanini explain in their 2020 book Humanocracy - Creating organizations as amazing as the people inside them.
‘Like Socio-Technical Systems, most of these initiatives were ultimately neutered, cloistered, or aborted’
– Gary Hamel and Michele Zanini
Though much admired, it ultimately couldn’t turn the wider tide of bureaucracy; its distinctive work practices “were steadily diluted”.
“Like STS, most of these initiatives were ultimately neutered, cloistered, or aborted”, Hamel and Zanini add.
They urge us to face facts about today’s bureaucracy:
Bureaucracy is familiar. You won’t have the courage to take on bureaucracy unless you believe there are alternatives. We must search out organisations that have successfully defied management orthodoxy
Bureaucracy is complex and systemic. Fragmented, half-hearted attempts won’t cut it. We need to replace the entire edifice of bureaucracy, one stone at a time.
Bureaucracy is well defended. There will be resistance, so management rebels need to join forces. You have to build a grassroots movement that can overwhelm or route around the defenders of the status quo.
Bureaucracy serves a purpose, however poorly. The goal is to carefully dismantle bureaucracy, not simply blow it up. You need a change strategy that is both audacious and prudent.
Bureaucracy is self-replicating. There will be no easy victories. Bureaucrats will fight back. To persevere, you’ll need a sense of purpose that’s as unshakeable as the path is arduous.
Potential next steps?
1. Support for Buurtzorg Britain & Ireland’s work to ‘support to NHS, social care and other organisations wishing to make changes inspired and informed by the Buurtzorg model’ is clearly a key way to help a shift to happen
2. Emerging efforts to create a Buurtzorg UK social enterprise, as a joint venture, could be crucial too, as well as developing a digital platform to match people in need to providers.

In your organisation, tools like The Ready’s Tensions and Practices cards can help make it easy for a team to start discussing and progressing potential moves in the direction of self-management and reduced bureaucracy.
3. Other self-managed/Teal organisations
There are a range of self-managed organisations outside the orbit of Buurtzorg Britain & Ireland. Here are the ones I’ve found (please let me know about others).
Wellbeing Teams
Wellbeing Teams have been a very visible approach in the UK, using small neighbourhood self-managed teams to offer “a radical new model for delivering care and support within communities”.
“The purpose of Wellbeing Teams is to do whatever we can to help people live well and be part of their community.”

It was founded in 2016 by Helen Sanderson MBE, and has been rated ‘Outstanding’ by CQC.
Wellbeing teams have used a variety of approaches: “from working in partnership with Local Authorities to deliver Wellbeing Teams as a local service provider, being commissioned directly by people with a personal budget or by providing learning and development for other organisations who want to learn about and use our approach.”
“At the time of our inspection the service was supporting 75 people with a regulated activity in Wigan, Lancashire and Abingdon, Oxfordshire”, say CQC. (NB CQC’s evaluation only covers regulated activities, not all of the work of Wellbeing Teams.)
“The service was in the process of starting to support people in Thurrock, Essex.”
CQC’s inspection findings include: “People said they knew their wellbeing workers well and that they went above and beyond what would normally be expected of them”.
“The service put the people they supported and the people who knew them best, at the heart of organising and planning care, so that the best outcomes for people were achieved.”
‘Paying home care for time-and-task is like only paying firefighters when they attend a fire’
– Helen Sanderson
CQC also found: “People were actively encouraged to maintain relationships with friends and remain active members of their wider local community and build new relationships. The service signposted people to events being run by other organisations and where a person’s interests were not being met, the service tried to arrange activities that would interest the person and link the person with a wellbeing worker who shared the same interest.”
Alas, Wellbeing Teams could not survive and thrive in current NHS structures: it was “killed by inflexible commissioning!”, as founder Helen Sanderson told me.
‘We lasted nearly 4 years; our key learning is that it takes innovative commissioning to support innovative providers’
– Helen Sanderson
“We were rated by CQC as outstanding but paying home care for time-and-task is like only paying firefighters when they attend a fire. We were committed to paying people whole shifts – like all other services except home care,” said Helen.
“We lasted nearly 4 years; our key learning is that it takes innovative commissioning to support innovative providers, so eventually we joined the fabulous Neighbourhood Midwives [see below], who were ahead of their time”.
“We are now working with providers and councils who want to use the principles and practices from Wellbeing Teams – this is exciting work.” (For example, supporting Camden Council to develop a self-managed team (for some of its Extra Care Housing), who would co-produce care with the residents. The team has to include a registered manager, for CQC purposes, but operates on a flat structure, with wellbeing workers, co-ordinators and community connectors “working together as equals to design and agree rotas, offer peer supervision and problem-solve together”).
Talking recently with people interested in setting up Wellbeing Teams she explained: “One of our most significant lessons was that innovative support providers need innovative commissioners and to find a way to share risk and learning”.
Neighbourhood Midwives
Neighbourhood Midwives was a pioneering model of midwifery services, based on a self-managing team and offering continuity of care (ie seeing the same midwife) around 500% better than found in the NHS.
In its own words, its midwives “offer personalised care throughout pregnancy, birth and beyond.”

“From convenient antenatal appointments at home and one-to-one care during labour (at home or in hospital), right through to those crucially important first four to six weeks with your newborn baby, your midwife is right by your side to provide all the advice, support and guidance you need as you settle into life with your new family.”
‘My midwives all still remember their Neighbourhood Midwives days as the one time they felt they really were able to practice midwifery as it should be’
– Annie Francis
“All the evidence shows that this type of care leads to better outcomes and greater satisfaction.”
Neighbourhood Midwives was highlighted as a promising new model in the NHS 10 year plan – thought subsequently quietly removed when it was forced to close, for familiar reasons. (Though it then offered a professional directory of independent midwives).
“My midwives all still remember their Neighbourhood Midwives days as the one time they felt they really were able to practice midwifery as it should be,” says its founder Annie Francis.
“They relished the individual and collective responsibility we all felt to the organisation, to each other and, most importantly, to the women and babies who trusted us. Everyone stepped up to the – many – challenges we faced because of the strong sense of purpose we had and the powerful partnership working our midwives developed with the women and families in their care.”
‘We did well in our CQC inspection, despite our processes being very different from what they were used to seeing in the NHS, the independent review of our pilot was positive and the feedback from the women was amazing’
– Annie Francis
“I still believe that the many benefits of a self-managing approach in public service work particularly well with midwifery because so much of what midwives do is based in autonomous practice and grounded in a social model of community care.”
“To be honest, I don’t think the closure of Neighbourhood Midwives was to do with the self-managing aspect,” Annie explains.
“We did well in our CQC inspection, despite our processes being very different from what they were used to seeing in the NHS, the independent review of our pilot was positive and the feedback from the women was amazing.”
‘What did for us was the commissioning structures and the finances’
– Annie Francis
“What did for us was the commissioning structures and the finances. When we tried to move on from our pilot to become integrated into the local health economy, the proposed plan was that the local maternity system (7 Clinical Commissioning Groups (CCGs) in total) should commission Neighbourhood Midwives teams – ideally one in each of the CCGs – which would have given us a sustainable number of teams/contracts. However, they all had to agree to this, apparently, and one was opposed, on the grounds that we were ‘private’. It was also started far too late in the day and we were out of step with the commissioning cycle but with no commitment from our CCG that they were able/willing to continue our contract in the meantime.”
“With no firm commitment to a future contract coming from anywhere we were caught in the cashflow challenge of any small organisation – which is why we had to close.”
“Financially, there were all sorts of reforms promised about how funding in the maternity services would change (part of the maternity transformation programme) as the payment by results did not work for anyone and particularly not for a small social enterprise with limited resources. These reforms moved at a glacial pace and were still nowhere near any sort of implementation when we closed.”
Neighbourhood Midwives were hit hard by insurance overheads too: “Insurance costs were huge too: we were charged at the same rate as the most high-risk NHS Trust – £1,000+ per birth – even though we were only contracted to work with low-risk women (our CCG being cautious). We also had to provide 5 years of claim history before they would consider reducing it and – although we had 5 years of zero claims if you include our private work – this wasn’t accepted…”.
“You get the picture I’m sure: there were just too many obstacles in our way to survive but they were to do with being a non-NHS provider plus the bureaucratic and interminably slow pace of change/reform, rather than our self-management per se. We had much more freedom to organise ourselves differently than NHS midwifery teams have – which I think stymies their ability to team-build and grow – but in the end the price was too high.”
BelleVie home care
Another Buurtzorg-inspired organisation – in Oxfordshire and Northumberland – is still-thriving BelleVie.
‘[Our] model allowed us to successfully test charging a monthly membership for outcomes and make that big break away from time-and-task’
– Trudie Fell
Founder Trudie Fell shares its journey: “we run a home care organisation using a Buurtzorg-inspired model of self-managing teams.”
“We started with self-funders after learning from Wellbeing Teams’ Helen Sanderson about the challenges of inflexible commissioning. This B2C (business-to-consumer) model allowed us to successfully test charging a monthly membership for outcomes and make that big break away from time-and-task.”
“We now cover most of Oxfordshire and do some work with the NHS there too. We launched in the North East where we found a council open to innovative ways of working and are piloting trust-based commissioning with them; 75% of our work in the NE is with the Local Authority.”
“We've made good use of tech to enable scale, co-designing and building our own Wellbeing OS tech platform with Teams. We learnt from Brendan that tech has been a consistent obstacle in his experience of Buurtzorg pilots in Britain. I'd be happy to talk about the highs and lows of our 4-year journey with our self-managing model: it's been a roller coaster!”
In 2023’s national Home Care Awards, BelleVie was a winner in four categories:
Most Outstanding Individual Home Care Provider
Best Palliative/end-of life care expertise
Innovative technology expertise
Best for Team Support Expertise (staff wellbeing)

In a January 2023 Linkedin post Trudie commented: “When 13,000 of our 100,000 hospital beds are occupied by elderly patients who have nowhere else to go, Rishi Sunak’s promise to fix NHS waiting times means we simply have to fix social care.”
‘In England, the best care workers often quit because they are not given the time to care for the whole person. The NHS treats social care as an afterthought. But if we saw care as a continuum, leading from public health through rehabilitation to supported housing and end-of-life, the job could be more rewarding, vocationally and financially’
– Camilla Cavendish
“Camilla Cavendish’s article in the Financial Times shows why BelleVie’s innovative model, proven to create an environment which values both those receiving and giving care, solves the problems our politicians face”.
“Camilla writes: ‘In England, the best care workers often quit because they are not given the time to care for the whole person. The NHS treats social care as an afterthought. But if we saw care as a continuum, leading from public health through rehabilitation to supported housing and end-of-life, the job could be more rewarding, vocationally and financially.’”
Paul Jansen added that we need to “stop seeing social care as the synonym for ‘care homes’, but as solutions in the community, in people’s own homes, in community hospitals and in care homes if and when most suited.”
Equal Care Co-op
Equal Care Co-op is the UK’s first platform-based social care and support co-operative.
‘Sociocracy allows groups with a shared aim or focus to self-organise, share ideas and information, and make decisions efficiently in a way that allows everyone to contribute’
– Marc Sweeney
“We are setting up the first self-managing peer group of care and support workers and community volunteers in the Calder Valley”, their website explains. North London is expected to follow.
Equal Care Co-op uses Sociocracy practices to support its self-management.
Marc Sweeney explains on their blog:
“Sociocracy allows groups with a shared aim or focus to self-organise, share ideas and information, and make decisions efficiently in a way that allows everyone to contribute. It utilises methods such as speaking in rounds and encourages the use of consent in decision-making – reaching a point where there are no objections and a decision is good enough for now or safe enough to try. This contrasts with the usual method of consensus, where a majority vote on something could overrule valid objections to it.”
‘This is a refreshing change for those who may occasionally struggle to speak up in meetings or feel that their managers sometimes ignore their suggestions and arrive at their own decision’
– Marc Sweeney
“It also flattens out the hierarchical structure often found in organisations. Those involved in a discussion are those directly connected to what is being discussed, and everyone is treated equally. Individuals are encouraged and given opportunities to contribute ideas that can effect real change. This is a refreshing change for those who may occasionally struggle to speak up in meetings or feel that their managers sometimes ignore their suggestions and arrive at their own decision.”
“Perhaps like me, you have previous experiences with two-hour meetings where it feels like nothing is being properly discussed or resolved. You may also have memories of sinking into your chair, barely getting a word in edgeways while others dominate the discussion. For me, learning that there's a different way that incorporates collaboration and active participation into its very structure, is exciting and eye-opening.”
‘Perhaps like me, you have previous experiences with two-hour meetings where it feels like nothing is being properly discussed or resolved… For me, learning that there's a different way that incorporates collaboration and active participation into its very structure, is exciting and eye-opening’
– Marc Sweeney
Equal Care Coop participated in the Care Quality Commission Sandbox (more on that below) – an attempt to reduce the barriers created by CQC’s inspection for novel, smaller care organisations.
Mayden
Mayden is a healthcare software company, mostly working with the NHS, that took the decision to move from hierarchical management to a ‘flat’ structure. It has 100+ staff and a turnover approaching £10m.

‘Why do we give adults a manager as if they’re children in need of supervision?’
– Alison Sturgess-Durden
Its journey is enjoyably shared in the 2023 book Made without Managers – One company’s story of a creating a self-managing workplace. Though the book is clear that it doesn’t want to offer a blueprint, it’s full of practical guidance around issues like promotion, cost-control, decision-making etc.
It’s always somehow refreshing too to hear the kind of ‘Emperor’s New Clothes’ type of fresh seeing that come from people who do work in flat, self-managed organisations: “Why do we give adults a manager as if they’re children in need of supervision?”
The gradual trend towards self-management has been a slow, steady indicator that there are better ways to address today’s turbulent environment than through expensive, lugubrious and soul-destroying bureaucracies and surveillance
– Margaret Heffernan
In the book’s foreword CEO and author of Wilful Blindness: Why We Ignore the Obvious at Our Peril, Margaret Heffernan writes: “The gradual trend towards self-management has been a slow, steady indicator that there are better ways to address today’s turbulent environment than through expensive, lugubrious and soul-destroying bureaucracies and surveillance.”
Chiltern Music Therapy
‘People often think self-managing teams is about a flat hierarchy, but really it’s about recognising people’s different strengths and providing an environment where people can take charge of the work they do’
Another self-managed organisation (and employee-owned too) that does work for the NHS is Chiltern Music Therapy: “We are an employee-owned, self-managing organisation. People often think self-managing teams is about a flat hierarchy, but really it’s about recognising people’s different strengths and providing an environment where people can take charge of the work they do, using advice from their peers, their professional judgement and life experiences to make informed decisions”, the organisation explains.
“We work in circles and pods and roles, not managers and teams.”
Elsewhere, three health boards in Wales received funding from the Welsh Government in 2018 to “to pilot neighbourhood nursing principles based on the Buurtzorg model of care” (more info).
Other parts of the UK with self-management initiatives include:
North Wales
Cornwall
South Downs Health and Care
Children’s services
The think-think/funder Centre for Public Impact – itself a self-managed organisation – teamed up with Frontline, a social work charity, and Buurtzorg Britain & Ireland to create ‘A Blueprint for Children’s Social Care – unlocking the potential of social work’.
The report argued that too many things get in the way of social workers’ ability to do their best work with families. They work in a bureaucratic environment, with excessive layers of management, oversight and process (‘too many eyes, not enough hands’), that has created a command-and-control culture which limits the positive impact they can make on a family’s life. They typically spend 29 hours a week on paperwork or at their PCs.

The blueprint showed how any local authority can redesign its children’s social care system in a way that increases the time social workers can spend with families and empower them to be able to make meaningful decisions for the children they work with, at no additional cost.
“What the blueprint represents however is not just a restructure, but a culture change in the way systems see and treat professionals, that is based on trust.”
Buurtzorg Britain & Ireland would eventually distance itself from the resulting blueprint, believing it had gone too far towards advocating a particular pre-existing structure as being the answer, rather than supporting the learning within the staff that would enable the organisation to develop a particular structure that would work for their own situation.
Covid interrupted interest from councils in taking up this approach.
Another organisation within the health and care space that – like the Centre for Public Impact – took the decision to become self-managing itself is the innovative consultancy Kaleidoscope Health & Care, founded by another fan of Frederic Laloux’s book Reinventing Organisations, Richard Taunt.
Kaleidoscope has been a self-managed organisation from its inception with three people, and now has 40 staff.
Social Care
The Care Quality Commission – often viewed as a bureaucratic obstacle to new ways of working – made a valuable attempt to open the door with its regulatory ‘sandbox’ project to develop a flexible regulated alternative for individual care and support at home workers.
Led by Simon Spoerer (from CQC’s Adult Social Care Policy Team), it sought to generate a proportionate new model for regulating micro care at home enterprises (more info; and here’s a Zoom about the sandbox).
The work was made possible by a grant from the £10m Regulators’ Pioneer Fund launched by The Department for Business, Energy and Industrial Strategy (BEIS) and administered by Innovate UK.
Elsewhere, the Cavendish report on Social Care highlighted the potential in taking Buurtzorg-style approaches: “My conviction that we can provide much higher quality, person-centred care while also saving money and ploughing that back into staff wages stems partly from my extensive knowledge of Buurtzorg, a not-for-profit home care provider in the Netherlands.”
Beyond health and care
South West-based We Care + Repair is ‘the largest independent home improvement agency in the UK’.
“Our aim is for people to live comfortably and independently at home for as long as they choose, enabling them to enjoy their lives in the surroundings they love. We are not for profit, which means any money that we make goes back into the organisation to support vulnerable people who cannot afford to pay for our services,” their website explains.
It is in the process of transitioning to become a self-managing/Teal organisation: “Currently focused on transitioning WE Care Home Improvements to a next stage, self-managing organisation and exploring new ways of working to establish effective collaboration between Health and Care and VCSE sectors to produce better outcomes for clients.”
It would be great to see some influential health and care-related organisations follow the lead of the Centre for Public Impact and Kaleidoscope Health & Care into self-management inside their own organisations
Potential shifts towards self-management/Teal crop can crop up in a wide range of places: St.Ethelburga’s Church in London – the ‘Centre for Reconciliation and Peace’ – for example, has talked about shifting to become a Teal organisation.
“How can we create cultures that make work productive, fulfilling and meaningful?”, one of their trainings asked.
“How can our organisations better mirror the values we want to see in the world? Inspired by the ground-breaking book by Frederic Laloux, join us for this practical, fun and participatory event exploring how alternative economic models can impact peace building and create systemic change.”
And We-Q is a “A team diagnostic survey tool that facilitates transformational conversations in the direction of the key teal breakthroughs: self-management, wholeness and evolutionary purpose.”
Not just an enabler of Teal/self-management, they also list themselves as also being an example of a Teal organisation.
“We-Q is a tool for transitioning from hierarchical management, through better management into true self management” – though case studies of organisations that have made this transition aren’t visible.
Other UK organisations have publicly talked about becoming self-managed/Teal but not so far chosen to follow through on it (eg RSA; see their public lecture with Frederic Laloux).
It would be great to see some influential health and care-related organisations follow the lead of the Centre for Public Impact and Kaleidoscope Health & Care into self-management inside their own organisations. If this happened, maybe a ‘tipping point’ could turn out to be far nearer than any of us are currently quite ready to believe…?
What I’ve not investigated for this article is the longer-established tradition of co-operatives. For example, the Community Counselling Cooperative CIC, in the North East, involves around 20 people. They make use of Seeds for Change’s free book A Consensus Handbook - Co-operative decision-making for activists, co-ops and communities.
And rather larger is Be Caring (formerly Care and Share Associates) which calls itself ‘the UK’s largest employee-owned social care provider’. In 2021 its 800 ‘co-owners’ (ie staff) provided “almost one million hours of care to 2,339 people across Leeds, Manchester, Liverpool and Tyneside”.
It also boasts a staff ‘Net Promoter Score’ of 62, a sign that its own staff would strongly recommend it to others as a good place to work.
Interestingly, Frederic Laloux argues that the ‘Teal’ self-managed organisations he spotlights seek to use quicker and more effective decision-making approaches than consensus, as focused on in the Seeds for Change handbook. (I don’t know how valid such a challenge is, and would love to hear from others who know more about it).
Self-management courses
A range of trainings to support teams and organisations moving into self-management are now available. For example:
Buurtzorg Building Blocks (6 session course) - Buurtzorg Britain & Ireland also offer bespoke training
Tuff Leadership (Tuff Self-Management – Employees and teams that manage themselves)
Trust Works (Moving Towards Self-Management)
New Ways of Working online course (Marc Eddleston)
The Hum (Patterns for Self-organising Teams)
Greater Than Academy (Practical Self-Management Intensive)
Corporate Rebels (Understanding and designing progressive organizational structures; How Buurtzorg works, Run Better Meetings etc)
Potential next steps?
A hub/clearinghouse for self-management/Teal materials for the NHS and social care might be valuable, and a fairly quick win.
It could include the latest research, case studies, websites, self-management trainings, commissioning innovations, a national map showing where self-managed organisations/services are located, links to communities of practice etc.
Reinvent commissioning
Support work such as Scotland’s ‘Commissioning Differently’ work to develop new models of commissioning that are more “person-centred, collaborative, trust-based and ethical” (current commissioning has restricted model’s like Cornerstone’s and contributed to the closure of pioneers like Wellbeing Teams and Neighbourhood Midwives).
4. Are NHS Integrated Care Systems (ICSs) an opening for self-management?
The NHS in England has (yet another) new structure, aiming to be a more cross-boundary structure, that brings together health and care. There are 43 of these Integrated Care Systems (ICSs) around England (Scotland had already sought to integrate health and care).
A recent Health Service Journal opinion piece on ‘The NHS’s ‘heartbreaking’ failure to innovate’ (6/12/22) by Lord Bethell and Lord Victor Adebowale found a ‘ray of hope’ in the NHS’s new integrated care structure: “It is not all doom and gloom and our hope is that ICSs, which are new and have a huge agenda ahead of them, can help to unlock the paralysis we are seeing”.

It's easy to see that such possibilities could potentially be unlocked for Buurtzorg-inspired services.
‘Integrated Care Boards create a more favourable institutional environment to enable people to work across the system at the practice level’
– Brendan Martin
The NHS-connected Good Governance Institute wrote about exactly this possibility in a piece on ‘The ICS case for the Buurtzorg nursing community care model’ (March 2021).
This rings true for Brendan, from Buurtzorg Britain & Ireland, too: “The new Integrated Care Boards create a more favourable institutional environment to enable people to work across the system at the practice level”.
“There’s more possibility for a holistic approach to care; more collaboration between organisations in the system”.
“But leaders have to have a sense that their role is to create the environment for those synergies,” he adds.
Current funding approaches often work against Buurtzorg-inspired models, because financial savings don’t appear in the required part of the system.
For example, Wendy Lansdown, who was part of the Buurtzorg team in Cambridge, shared that it didn’t demonstrate the necessary level of savings to the county council. It did, however, evidence good savings to the wider system.
Perhaps the larger, integrated footprint in the NHS will make it easier to recognise and value such savings to the wider system?
“I think there’s new potential where the partnerships and shared purpose/values are strong”, said Wendy.
Conclusion
As most people would probably agree, the case for self-managed (Teal) organisations like Buurtzorg in the NHS and beyond remains as compelling as ever: higher quality care, a more rewarding workplace, with less bureaucracy and cost. It also builds community and resilience, which is increasingly seen as vital.
‘Although the national policy agenda and government statements call for a more personalised care and outcomes-based approach to care, the system is lagging in delivery of these expectations… most homecare commissioned by local authorities is still delivered on a time and task model’
– Karla Zimpel-Leal
And – as mentioned at the start – business academic Mark Thompson back in 2015 made a quick estimate that a self-managed approach could save £35.5bn across Britain’s public sector, freeing up thousands of staff to return to valuable frontline work.
Patients themselves increasingly want this kind of care: staying at home, with continuity of care rather than ‘time and task’ with different faces turning up day in, day out.
But the health and care system is lagging in offering this, as Karla Zimpel-Leal explains: “Although the national policy agenda and government statements call for a more personalised care and outcomes-based approach to care, the system is lagging in delivery of these expectations. On a practical level, most homecare commissioned by local authorities is still delivered on a time and task model. Innovative models appear to offer a closer match to users’ needs and expectations.”
With an ageing population it’s particularly important to be offering these services that people want (and can keep them in their homes and communities) more widely.
If we are to see Buurtzorg-inspired initiatives spreading, rather than too often stymied or closed, effort needs to be put into reforming commissioning (and its accompanying targets/outcomes) so that it can become an enabler rather than a barrier.
When no Buurtzorg-inspired initiative is on the agenda or seems possible, NHS organisations can – arguably – still benefit from a range of energising kindred approaches that I think/hope might pave the way to a more autonomous/self-managed approach, that’s also more place-based, person-centred and strengths-based – to use use the current jargon.
I discuss a range of such potential kindred approaches in part 2 of this article – coming soon. And also discuss such potentially relatively straightforward levers for change as the deliberate recruitment of more transformative ‘Teal’ leaders, to help the NHS to make quicker strides forward (as was successfully once done when recruiting a new Chief Executive for Swindon Council).
Further reading
Binder, Thomas (2023), Ego Development for Effective Coaching and Consulting - Including a Comprehensive Overview of Ego Development Theory, its Validation, Critique and Empirical Foundations (Vandenhoeck & Ruprecht).
Bunting, Michael with Lemieux, Carl (2022), Vertical Growth – how self-awareness transforms leaders and organisations (Wiley).
Bushe, Gervase (2020), The Dynamics of Generative Change (BMI Series in Dialogic OD).
Cabraal, Anthony and Basterfield, Susan. (2018). Better work together – How the power of community can transform business (Enspiral Foundation).
Capelle, Ronald (2014), Optimising Organization Design - a proven approach to enhance financial performance, customer satisfaction, and employee engagement (Jossey-Bass) [Elliot Jaques-based ‘Requisite’ approach to organisation design - not self-management - discussed further in part 2].
Cavendish, Camilla (2022), Social care: Independent report by Baroness Cavendish – How can we lock in the lessons of the crisis to build a more robust, sustainable, joined-up system of health and social care? (PDF).
deBruin, Jeanine, Doodkorte, Remco and Sinervo, Timo (2022), ‘The implementation and outcomes of self-managing teams in elderly care: A Scoping review’, Journal of Nursing Management.
Demick, Jack and Andreoletti, Carrie (Eds.)(2003), Handbook of Adult Development (Springer).
Dignan, Aaron, (2019) Brave New Work: are you ready to reinvent your organization? (Penguin).
Dobie, L, Howlett, D, Reid, E, & Murray, A (2019), Improving patient outcomes with neighbourhood care: The Coldstream experience. British Journal of Community Nursing, 24(10).
Drath, Wilfred H, (1993), Why Managers Have Trouble Empowering: A Theoretical Perspective Based on Concepts of Adult Development (Report no. 155, Centre for Creative Leadership).
Drennan, V, Calestani, M, Ross, F, Saunders, M, & West, P (2018), ‘Tackling the workforce crisis in district nursing: Can the Dutch Buurtzorg model offer a solution and a better patient experience? A mixed methods case study’. BMJ Open, 8(6).
Drennan, V, Ross, F, Calestani, M, Saunders, M, & West, P (2018), Learning from an early pilot of the Dutch Buurtzorg model of district nursing in England. Primary Health Care, 28(6).
Drennan, V, Ross, F, Saunders, M, & West, P (2017). The Guy’s and St. Thomas’ NHS Foundation trust Neighbourhood nursing team test and learn project of an adapted Buurtzorg model: An early view (pdf).
Eddleston, Mark (2022) New Ways of Working Playbook
[Note: these curated online resources cover meeting structures, decision-making, roles, conflict-resolution, agreements etc; pdf].
European Regional Development Fund (2023), Transforming Integrated Care in the Community (TICC) - Blueprint (pdf).
European Regional Development Fund (2023), Transforming Integrated Care in the Community (TICC) - Evaluation Report 2017-2022 (pdf)
Francis, Annie (2020). Neighbourhood Midwives: The model that boosted continuity of care by 500% – with Annie Francis [Zoom recording on Youtube].
Gill, Lisa, Leadermorphosis podcast
[Note: Lisa’s great self-management-oriented podcasts include everyone from Edel Harris (Cornerstone) to Gary Hamel and Amy Edmondson, and self-managed orgs like Buurtzorg (eg Jos de Blok on the virtues of humanising, not protocolising), Mayden, Haier, Percolab, Nearsoft and many more.]
Gray, B. H., Sarnak, D. O., & Burgers, J. S. (2015). Home care by self-governing nursing teams: The Netherlands’ Buurtzorg Model (Vol. 14). The Commonwealth Fund.
Hamel, Gary and Zanini, Michele (2020). Humanocracy: Creating Organizations as Amazing as the People Inside Them (Harvard Business Review Press).
Hamm, C., & Glyn-Jones, J. (2019). ‘Implementing an adapted Buurtzorg model in an inner city NHS trust’. British Journal of Community Nursing, 24(11).
Hanley, Joe, McGrath-Brookes, Michael and Higgins, Martyn. (2021). ‘Dismantling the Blueprint: Buurtzorg in English child protection social work’, European Journal of Social Work.
Harris, Edel (2019). Radical Models of Organising – Edel Harris [recording from Next Stage Radicals conference, London] Youtube.
Healthcare Improvement Scotland. (2021). Community-led models: Innovation in health and social care – Learning from new approaches in Scotland and the UK (PDF).
Healthcare Improvement Scotland. (2019). Learning from neighbourhood care test sites in Scotland (PDF).
Hoare, Carol (ed.)(2011) The Oxford Handbook of Reciprocal Adult Development and Learning (Oxford University Press).
Johansen, F., & van den Bosch, S. (2017). ‘The scaling-up of neighbourhood care: From experiment towards a transformative movement in healthcare.’ Futures, 89.
Jantunen, S., Piippo, J., Surakka, J., Sinervo, T., Ruotsalainen, S., & Burström, T. (2020). ‘Self-organizing teams in elderly Care in Finland: Experiences and opportunities’. Creative Nursing, 26(1).
Joiner, Bill and Josephs, Stephen (2007) Leadership Agility – Five Levels of Mastery for Anticipating and Initiating Change (Jossey-Bass).
Kamara, Yamin, Rodriguez, Cendrig and Moyo, Nokuthula (2022) ‘District nursing using neighbourhood care principles in practice: reflecting on our experience’, British Journal of Community Nursing, Nov.
Kegan, Robert (2013), The Further Reaches of Adult Development (YouTube).
[Note: I invited Prof Kegan to give this RSA lecture in London, where he spoke about how the world needs more of the Self-Transforming/Teal mind, as it uniquely capable of truly listening to all the stakeholders involved in the world’s ‘wicked’ problems].
Kegan, Robert, Lahey, Lisa et al. (2016) An Everyone Culture – Becoming a Deliberately Developmental Organization (Harvard Business Review Press).
Kreitzer, M. J., Monsen, K. A., Nandram, S., & De Blok, J. (2015). Buurtzorg Nederland: A global model of social innovation, change, and whole-systems healing. Global Advances in Health and Medicine, 4(1).
Lalani, M., Fernandes, J., Fradgley, R., Ogunsola, C., & Marshall, M. (2019) Transforming community nursing services in the UK; lessons from a participatory evaluation of the implementation of a new community nursing model in East London based on the principles of the Dutch Buurtzorg model’. BMC Health Services Research, 19(1).
Laloux, Frederic. (2014) Reinventing Organizations – a guide to creating organizations inspired by the next stage in human consciousness (Nelson Parker).
Laloux, Frederic (2016) Reinventing Organizations – an illustrated invitation to join the conversation on next stage organisations (Nelson Parker).
Leask, CF, Bell, J and Murray, F, (2020) ‘Acceptability of delivering an adapted Buurtzorg model in the Scottish care context’, Public Health, 179.
Leask, C. F., & Gilmartin, A. (2019). ‘Implementation of a neighbourhood care model in a Scottish integrated context-views from patients’. AIMS Public Health, 6(2).
Leask, Calum and Macleod, Sandra (2023), ‘Exploring the implementation and evaluation of a distributed leadership model within a Scottish, integrated health and care context’, BMJ Leader (pdf).
Lee, Michael and Edmondson, Amy. (2017) ‘Self-managing organizations: Exploring the limits of less-hierarchical organizing’, Research in Organizational Behavior.
Lowe, Brent, Basterfield, Susan and Marsh, Travis (2017). Reinventing Scale-ups – Radical Ideas for Growing Companies – Beta 2.0. (ReinventingScaleUps.com).
Maurits, E. E. M., de Veer, A. J. E., Groenewegen, P. P., & Francke, A. L. (2017). ‘Home-care nursing staff in self-directed teams are more satisfied with their job and feel they have more autonomy over patient care: A nationwide survey’. Journal of Advanced Nursing, 73(10).
Martin, Brendan et al (2023) ‘Could Buurtzorg work in Britain?’ (YouTube)
(Zoom recording about 2023 Transforming Integrated Care in the Community report; includes two members of UK Buurtzorg-based teams).
Mascolo, Michael and Bidell, Thomas (Eds.) (2020) Handbook of Integrative Developmental Science: Essays in Honor of Kurt W. Fischer (Routledge).
Maybin, Jo et al (2019), A review of the West Suffolk Buurtzorg test-and-learn in 2017–18 (The King’s Fund).
McGuire, John and Rhodes, Gary. (2009) Transforming Your Leadership Culture, (Centre for Creative Leadership).
Mezey, Matthew Kalman (2015), ‘Planting the Seeds of New Possibilities: The Journey that led me to Reinventing Organization’ (interview with Frederic Laloux on Enlivening Edge website)
Mezey, Matthew Kalman (2015), ‘The Hot Management Trend of Self-organising Workplaces without Managers: will Left or Right be first to embrace it?’ (article on Enlivening Edge website).
Minnaar, Joost and de Morree, Pim. (2020). Corporate Rebels – Make work more fun (Corporate Rebels Nederland B.V.).
Monsen, K., & de Blok, J. (2013). ‘Buurtzorg Nederland’, The American Journal of Nursing, 113(8).
Monsen, K. A., & de Blok, J. (2018). ‘Buurtzorg: Nurse-led community care’, Creative Nursing, 24.
Nandram, S., & Koster, N. (2014). ‘Organizational innovation and integrated care: Lessons from Buurtzorg’. Journal of Integrated Care, 22(4).
Narayan, M. C., Tennant, J., Larose, P., Grumbly, J., & Marchessault, L. (1996). ‘Achieving success in home care: Through the self-directed work group approach’, Home Healthcare Nurse, 14(11).
Nixon, Tom. (2021). Work with Source – Realise big ideas, organise for emergence and work artfully with money (Work with Source).
Ostergaard, Erik Korsvik. (2020). Teal Dots in an Orange World – How to organize the workplace of the future (LID Publishing Ltd).
Perez, Matt, Perez, Adrian, and Leal Adrian (2021), RADICAL COMPANIES: Organized for Success without Bosses or Employees (Pradera Media).
Petraki, Mini and Brown, Andrew. (2019). Learning from the implementation of the Maternity Pioneer Programme in East London [Neighbourhood Midwives After Action Review meeting report] (NEL/NHS).
Pflaeging, Niels. (2014). Organize for Complexity – How to get life back into work to build the high-performance organization (BetaCodex Publishing).
Reams, Jonathan (2020), Maturing Leadership – how Adult Development Impacts Leadership (Emerald Publishing Limited).
Richards-Green, Shannon, Gough, Suzanne and Mickan, Sharon (2023), ‘Leadership at the intersection of healthcare and constructive developmental theory: a scoping review’, Asia-Pacific Journal of Health Management 18(2).
Robertson, Brian. (2015). Holacracy – The revolutionary management system that abolishes hierarchy (Penguin Random House).
Rooke, David et al. (2015). The hidden talent: Ten ways to identify and retain transformational leaders (PwC/OSCA).
Rooke, David and Torbert, Bill. (2005) ‘Seven Transformations of Leadership’, Harvard Business Review (April). (PDF)
Rooke, David. (2018) ’Transformational leadership capabilities for medical leaders’, BMJ Leader; 2:3-6. (PDF).
Rowson, Jonathan, Mezey, Matthew Kalman and Dellot, Ben (2012), Beyond the Big Society - Psychological Foundations of Active Citizenship (RSA).
Shepard, Ken et al (2007), Organization Design, Levels of Work & Human Capability – Executive Guide (Global Organization Design Sociey)
[Note: my review of this book is here http://integralleadershipreview.com/5282-book-review-organization-design-levels-of-work-human-capability-executive-guide/]
Slade, Samantha. (2018) Going Horizontal – creating a non-hierarchical organization, one practice at a time (Berrett-Koehler).
Slocock, Caroline (Ed.) (2018) Insights for a Better Way – Improving services and building strong communities (Civil Exchange/Carnegie UK Trust/Esmee Fairbairn Foundation).
Spoerer, Simon (2020), CQC reimagining the rules: supporting new ways of providing social care support – with Simon Spoerer.
[Zoom about CQC’s ‘sandbox’ project, which aimed to develop a flexible regulated alternative for individual care and support at home workers]
Sprinks, J. (2014). ‘Netherlands district staff turn their backs on bureaucracy’. Primary Health Care, 24(9).
Team Mayden, Sturgess-Durden, Alison, Kindon, Dr Philippa, and May, Chris (2023), Made without Managers – One company’s story of a creating a self-managing workplace (Right Book Company).
Tenelius, Karin and Gill, Lisa. (2020). Moose Heads on the Table – stories about self-managing organisations from Sweden (TUFF Leadership Training).
Timms, Perry (2020). The Energized Workplace: Designing Organizations where People Flourish (Kogan Page).
Torbert, Bill and Associates. (2004). Action Inquiry – The Secret of Timely and Transforming Leadership (Berrett-Koehler).
Vannucci, Delfina and Singer, Richard (2010), Come Hell or High Water – a handbook on collective process gone awry (AK Press).
Vermeer, A, Wenting, B. (2018) Self-management: How it does work (Bohn Stafleu van Loghum).
Voronov, Maxim and Yorks, Lyle (2015), ‘“Did You Notice That?” Theorizing Differences in the Capacity to Apprehend Institutional Contradictions’, Academy of Management Review, Vol. 40, No.4.
Wageman, R. (1997). ‘Critical success factors for creating superb self-managing teams’, Organizational Dynamics, 26.
Wilson, Richard, Mezey, Matthew Kalman and Nielsen, Nick (2013). Anti Hero - the Hidden Revolution in Leadership & Change (OSCA).
Yeatts, D. E., & Seward, R. R. (2000). ‘Reducing turnover and improving health care in nursing homes: The potential effects of self-managed work teams’, Gerontologist, 40(3).
Zimpel-Leal, Karla. (2021). ‘Emergent homecare models are shaping care in England: an ethnographic study of four distinct homecare models’ in Hefner, J.L. and Nembhard, I.M. (Ed.) The Contributions of Health Care Management to Grand Health Care Challenges (Advances in Health Care Management, Vol. 20), Emerald Publishing Limited.